


This is the third in a series of blogs on advocacy topics as we enter into the prime advocacy period of the year.
- ME/CFS Experts Speak Out in #MEAction’s Long Covid Media Conference
- Time to Strike! Sign Up for a Monumental Virtual Lobby Day
“America’s Hidden Health Crisis” – CDC.
The stats are striking. A bit horrifying, to be sure – but certainly very striking.
- Chronic fatigue syndrome is more debilitating than many chronic diseases including multiple sclerosis, chronic renal failure, congestive heart failure, lung cancer, stroke, and type-2 diabetes.
- As many as 75% of patients are unable to work.
- An estimated 25–29% are homebound or bedbound.
- ME/FS costs the U.S. $18–24 billion in lost productivity and medical costs a year.
- Recovery rates are at about 5%.
- There are fewer than 2 dozen nationally recognized experts in the U.S.
We’re not talking about a sore throat here! Art Mirin, Mary Dimmock and Leonard Jason lay it out all so clearly in their 2020 blockbuster paper, “Research update: The relation between ME/CFS disease burden and research funding in the USA” . The study updates a 2016 piece which, for the first time, attempted to apply a crucial epidemiological statistic – disability adjusted life years (DALYs) – to ME/CFS.
DALYs were developed in the 1990s to get a more accurate measure of a disease’s true burden. Chris Murray’s commitment to use them to illuminate the true state of the world’s health led Bill Gates to fund the $125 million Institute for Health Metrics and Evaluation (IHME). Since then the IHME has become the most trusted institution regarding disease burden in the world.
DALYs, then, are crucial statistics for any disease – and that hasn’t really sat well with an institution which doesn’t consider disease burden at all when giving out funding. A 2011 study suggested that only a third of the National Institute of Health’s (NIH’s) funding could be accounted for by assessing disease burden. Two thirds of it was being produced by something else.
By 2015, the NIH, which with its $43 billion/year budget, is easily the biggest medical research funder in the world – had gotten so hammered by questions about where its funding was going that it produced a report. The results were a mishmash. The NIH was pumping lots of money into some of society’s most destructive disorders and was missing the boat on others. In general, the results weren’t great or terrible – they were kind of in-between.
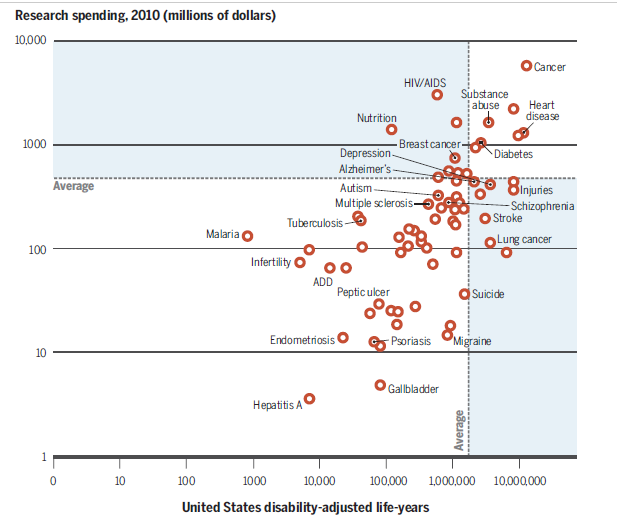
Some really ugly facts cropped up in those results. Emphysema, the third leading cause of death in the U.S., gets paltry funding compared to HIV/AIDS – which gets no less than 10% of the NIH’s entire research budget. Despite the fact that migraine actually poses more of a disease burden than HIV/AIDS in the U.S., it was getting more than a thousand times less funding.
Chronic fatigue syndrome (ME/CFS) was not included. This wasn’t the NIH’s fault, but it underscored – if it needed underscoring – just how penalized poorly studied diseases are – you can’t even get on the darn map. Just getting accurate DALYs for ME/CFS, however, required having epidemiological statistics that ME/CFS doesn’t have. As Mirin, Dimmock and Jason noted:
“The calculation of DALY for ME/CFS in this study is significantly limited by the lack of research and the poor quality of epidemiological studies assessing the natural progression of the disease, the prevalence of the disease overall and at different levels of severity, the corresponding levels of disability, and the magnitude and timing of premature death due to the disease and its complications.”
Still, you do what you can, and the Mirin-Dimmock-Jason 2020 update, “Research update: The relation between ME/CFS disease burden and research funding in the USA, of their 2016 study suggested that ME/CFS would have stuck out like a sore thumb. In it, the authors did a very clever thing: if the NIH didn’t include ME/CFS in their funding and disease burden assessment, they would.
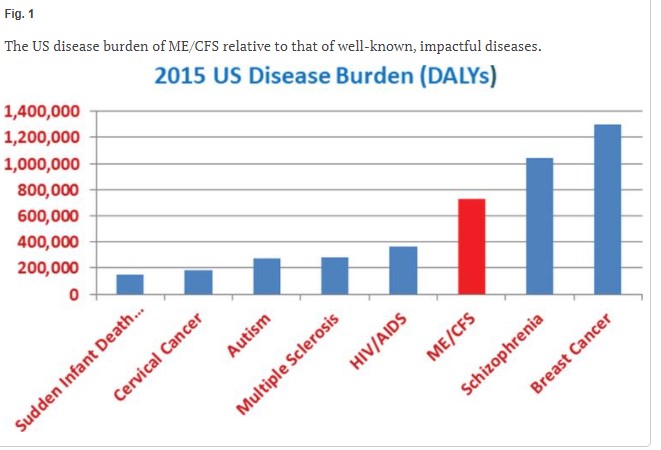
First came the disease burden (DALY) which, besides mortality, includes years of healthy life lost by being in poor health. Note that diseases which strike earlier, such as ME/CFS, will have higher disease burdens because more “years of healthy life” will be lost. The study found that the disease burden ME/CFS imposed was over double that of multiple sclerosis and much higher than HIV/AIDS.
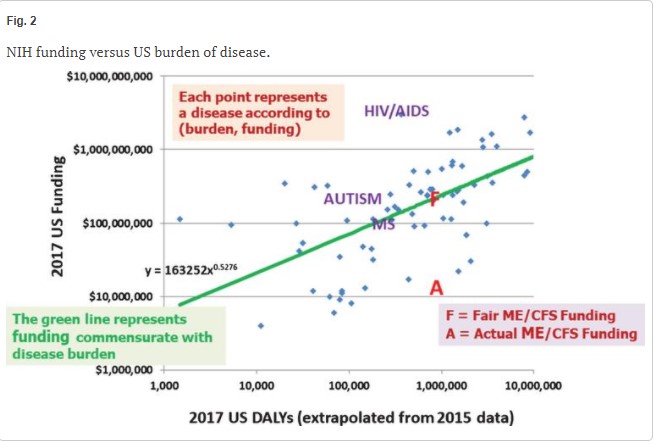
Next – comparing NIH funding with the burden produced by ME/CFS indicated that ME/CFS had one of the higher levels of disease burden – and one of the lowest levels of funding (A). Using the NIH’s own plot, the authors estimated that NIH funding would have to increase 14x’s to well over a hundred million dollars to be commensurate with the burden ME/CFS wreaks on people in the U.S.
Next, they asked how ME/CFS fared funding-wise compared to diseases with similar disease burdens.
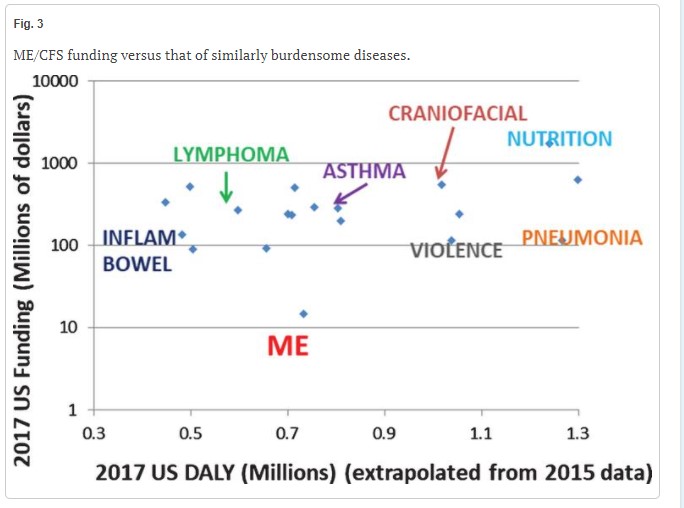
Funding for diseases with similar disease burdens.
Ouch! ME/CFS is sitting way at the bottom with the least amount of funding. The situation is actually much worse than it looks. Since the data is plotted on a logarithmic scale, ME/CFS isn’t even close to getting the amount of funding than, other diseases which produce similar disease burdens. Inflammatory bowel disease and asthma, for instance, get over 10 times the funding that ME/CFS does.
Next they asked what percentage of funding each disease was getting if it were funded at the expected levels, given its disease burden.
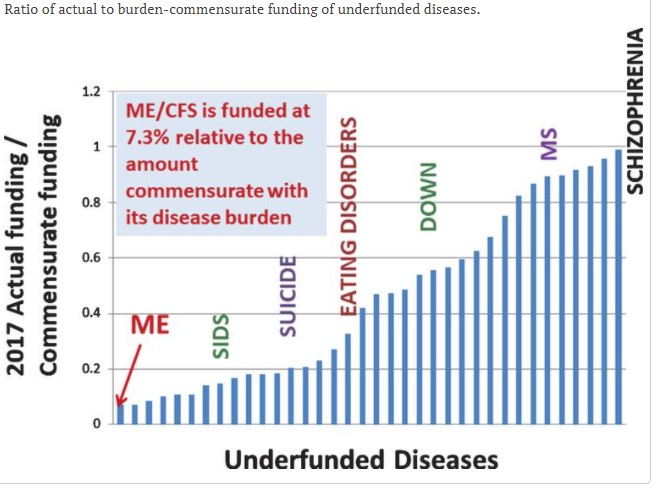
Percentage of funding relative to that expected, given a diseases disease burden.
Once again, ME/CFS demonstrated an uncanny ability to be at the very bottom of the barrel.
Next Step
One could (and will) gnash one’s teeth, beat one’s chest and just generally groan at the lack of support provided by the NIH. The trick, though, is not to give into despair or even anger. The consequences of giving into the despair is that nothing ever does change. You do get to spare yourself the risk of trying to make a difference, but the lousy funding, little support, few doctors … that will stick around – and who really wants that? You might as well get into action.
The good news is that wehave a really, really, (really) strong case to make. The only things that I can see that have moved the NIH with respect to ME/CFS are Congress and NIH-originated reports (IOM, Pathways To Prevention report).
The NIH is difficult to directly intervene with. Its response to the hundreds of media reports on the long haulers was to basically ignore them. It was not until Congress gave the NIH over a billion dollars to study the long haulers that the NIH actually started to do something about them.
Congress, though, is another story. Congress gets it that there’s something wrong about providing peanuts to a disease that affects a million-plus people. There’s something immoral about funding a disease at 1/14th of what its disease burden indicates it should get.
Plus, Congress is the elephant in the NIH’s room. Congress yields a big stick – it funds the NIH. It turns out that, historically, it’s Congress that’s been the big mover at the NIH. Most major NIH initiatives (Brain Initiative, HEAL Initiative, 21st Century Cures) originated in Congress – not the NIH. If we can really get Congress on our side, the NIH’s history of neglect is over.
We don’t need to despair at those evocative graphs. They’re providing sweet tools for making our case. Our most potent opportunity to do that is coming up at Solve ME/CFS Initiative’s Lobby Day/Lobby Week.
On Lobby Day, we get to talk to the only people who can push the NIH around. Lobby Week goes from April 18th to the 24th. Representative Jamie Raskin will be giving a keynote address.
Make a difference – participate in Lobby Day.
Register Here Before April Sixth To Make a Difference.
A big thank you to Art Mirin, Mary Dimmock and Leonard Jason for providing such evocative snapshots of where we are.
Coming up:
- The Education of an Advocate
- The NANDSC Report – Did it Make a Difference?
- The Continuing Hunt For Funding
















I’d like to see a documentary done on this. The scandal, The people holding us back exposed. PACE trial lies. The resulting lack of funding. Tge pathetic disease name. The years of suffering because of these politics
And importantly the reason why there’s now still no treatment for Long Covid sufferers. They need to know why too!!
Had this disease been taken seriously, there could well be good treatments available now. But instead millions more had to suffer before anything was done. And ME/CFS is still being overlooked!
Take information from David Tuller’s book ‘Trial by Error’ and a few other investigative books and ME journalists. And boom we’d have one of the most interesting documentaries out there. An actual real life conspiracy story.
It will open knowledge of ME/CFS up to the public, and the result will be political pressure and more funding
Show the heroes too, Ron Davis, OMF Whitney Dafoe, David Tuller, Jennifer Brie, Linda Bateman, Nancy Klimas, Jarred Younger, ‘Solve ME/CFS’ And many more of those that fought for us. Including you Cort Johnson
It would be a gripping and fantastic documentary that I’d donate to if you set up a fund page Cort?
No kidding. What a great story…Look at the difference that Osler’s Web made. We could use another Osler’s Web as a book or a film or hopefully both.
We’d have to find someone to do it. I can’t – too busy with the website. Can’t keep up with things as it is.
David Tuller would be the guy I would think 🙂
Ron and Whitney’s story alone is magnificent. He was just interviewed on People!
https://people.com/health/scientist-ron-davis-son-chronic-fatigue-syndrome/
I’ll ask my brother for advice, as he is a known person in the international film industry, as he works beside the likes of Peter Jackson. He’s often hired to edit their films.
He is probably too busy to do the documentary though, as is in New Zealand, where filming is ramping up due to no community Covid here.
But he’d give us fantastic advice as he has done quite a few documentaries other the years.
He’d probably know a few film industry people looking for work as things are reasonably quite for them due to Covid. They might not be asking for as much money as they used to either!
I am so grateful to Prof Ron Davis and others for their research which gives us hope. A condition that has robbed me of enjoying the life l used to have way too long. I rode race horses, worked for an airline, travelled the world, jumped off a mountain in a hang glider in France, love painting and dancing. Years of pain because l kept trying to do more than my body could cope with …trying to be me again ! All this while being mocked by the medical professionals and the media !
I think you’re absolutely right Brendan Rob – it’s an incredible scenario isn’t it? I can’t see how the pitiful treatment of millions of people can continue to go unnoticed, when there seems to me to be such momentum building. But it’s about keeping up that relentless pressure.
solveCFS is not even mentioning ME/CFS in ME/CFS Advocacy Week talking points. If our own advocacy group thinks it is ok to erase us – why would anyone else pay attention.
We know we can’t get $100 million to increase medical education, provide better training for doctors and set up patient registries for ME/CFS. That’s not even close to being possible. But we can get the big bucks for long COVID – and since long COVID in large part is ME/CFS – by doing that we are strengthening ME/CFS. LPlus post-infectious illnesses – of which ME/CFS is the major one – are included in the ask.
This is not about erasing anything- it’s about being strategic. Its clear that many long COVID patients are just like people with ME/CFS. By building the infrastructure around them we are inevitably helping us.
I think one of the problems with the documentaries done so far is that they have been, well, for lack of better word, “whiny” and come across as self-pitying. Any documentary would have to be more compelling on a fact basis than the ones have to date, which have been pretty cringe-worthy. No, I cannot do one.
Sticking to the facts and the numbers, though, is a really good strategy.
One of my doctors told me last week that what ME needs is for a super rich multi-billionaire to come down with it, and fund a ton of research. Any candidates out there?
As I recall, what lured the senior Bill Gates to give Cystic Fibrosis $20 million in the late l980s (see New Yorker article ca 1996) was that there was the promise of research finding treatments or a cure through beginning genetic research.
What do we have to lure a senior Bill Gates to fund us? One thing would be a major research capability. Would one of the regional centers qualify? Good to keep pressing on NIH but I really doubt that is where the breakthrough is going to come from.
Check out the New Yorker article about early funding for CF research; it’s really interesting. It was most definitely NOT from the federal government!
Yep. Totally agree with you Cameron. Especially after the PACE-Gate accusations of MECFS patients being ‘difficult’ and angry, whiny and self-pitying isn’t a good look. Especially when the data pretty much speaks for itself, and makes the case for us.
The sad thing is, most MECFS people I know are not especially whiny nor self-pitying (well, not beyond what the actual rubber-hits-the-road challenges would rightfully elicit). Most of us are pretty stoic, all things considered.
Fibromyalgia, with multiples of the number of sufferers compared to ME, is not even charted there. Long Covid will fund ME but the rest of us will die in pain with FM.
Yes, fibromyalgia is not there either. Nor when I checked a couple of years ago was the IHME tracking it. I specifically asked them how they could ignore a disease which affected about 10 million people. They didn’t answer. I would be surprised, actually, if enough epidemiological data was there to produce DALY’s for FM, but Steve please don’t despair. I would be shocked if long COVID didn’t lift both ME and FM. Planning to do a blog on that.
Yes, I agree with Steve. Fibromyalgia is almost identical to ME/CFS and yet doesn’t even get a mention. Many of us are bed and housebound and cannot work. To be continually ignored and misunderstood makes our plight feel more hopeless than ever.
PS to my comment above re finding a research base for ME: note that Cystic Fibrosis is not even mentioned on the charts in Cort’s summary. CF kills children, shortens life span, and causes lifelong disability from birth. There is a ton of research being done now: funded by the Cystic Fibrosis Foundation (CFF) and its offshoots. Probably a better model for ME (including FM, the boundaries between the two so indistinct most of the time) than the NIH model.
A problem ME/FM patients share with HIV, though, is the frequent lack of family support. The CFF nurtures and receives tons of family support in fundraising.
One of the things that struck me about “Straight Talk from Carole Head” interview – and which still strikes me – was the lack of support from people just outside the inner sphere of ME/CFS – people who can and do whip out $1 or $10 million contributions. Even Carole’s close friends would not provide significant contributions. We’re missing a huge swath of really wealthy people – the kind of people who give heavily to causes.
They will come eventually. Maybe COVID-19 long haulers will open their hearts and minds and their pocketbooks. What a worthy cause to support!
https://www.healthrising.org/blog/2019/07/27/straight-talk-carol-head-solve-me/
The ME/CFS underfunding is even more extreme in an analysis of 2015 burden versus 2019 funding, as seen in my paper Gender Disparity in the Funding of Diseases by the US National Institutes of Health – https://www.liebertpub.com/doi/10.1089/jwh.2020.8682 – where we estimate the 2019 burden-commensurate funding to be $246M (compared to $15M actual). Also, my recent paper with Lenny Jason – Updating the National Academy of Medicine ME/CFS prevalence and economic impact figures to account for population growth and inflation – https://www.tandfonline.com/doi/full/10.1080/21641846.2021.1878716 – estimates annual economic impact of ME/CFS in US to be $36-51B (vs the NAM figure of $18-24B).
These numbers can be upsetting but they also enable us to make a really good case for action – so bring them on. Thanks Art for all the work you’ve done.
Cort, apparently you are not aware that years ago, Congress included a line item in the budget allocating about $5 million to CFS research. This was prior to this century, maybe the 80s? Anyway, the Congress sent that over to NIH, who promptly spent it ALL on something else. Male pattern baldness or something equally TRIVIAL. So having Congress “on our side” doesn’t make any difference whatsoever to the NIH.
Hi Kate, you have bits and pieces of the story. In the late 1990’s I believe it was we had a champion in Congress who got Congress to allocate money to the CDC for ME/CFS. The CDC promptly redirected it to other purposes.
https://www.washingtonpost.com/archive/politics/1999/08/06/retaliation-alleged-at-cdc/c3ea5fdd-fc7f-4cd1-8dbf-c42e76f75c7f/
Bill Reeves who worked on the CFS program apparently internally questioned where the money went, was then given poor evaluation ratings, which lead him to file for whistleblower protection. He then blew the scheme out into the open. An Inspector General ultimately found that a Director Mahy had diverted almost $13 million in funds to other illnesses. He also found that the CDC had lied to Congress about where the money went.
The CDC had egg on its face, Mahy was reassigned, the CDC returned the money to ME/CFS and launched a public relations campaign on behalf of ME/CFS. Around that time I think CFSAC became a formal structure and ME/CFS was given it’s own grant review panel.
One of the morals of the story -was that whatever you do – don’t lie to Congress. Once Congress starts controlling the money the NIH is spending on ME/CFS they’re going to ask for regular reports. (That’s standard procedure.) They and we can use those to show how ME/CFS’s needs are or are not being met.
It actually ended up being quite a win for ME/CFS!
Also, I don’t understand how Jason et al came up with 100 million as the appropriate level of funding for CFS. The first part of the article points out that the disease burden is higher than that of HIV/ AIDS, so that tells us CFS should receive MORE funding than HIV/AIDS. But that disease is funded in the billions of dollars and has been for decades. Why should ME/CFS be funded less than a disease with a lower burden?
The thing with HIV/AIDS is that it receives way MORE money than its disease burden suggests it should. It’s an outlier.
The place to look for the appropriate funding is on the slanting area which delineates that average disease funding per disease burden.
New Japanese study out, finding ‘skewed’ B cell receptors in CFS.
I am not sure what that means, but it’s clearly some sort of dysfunction in the b cells.
Perhaps the Norwegians were on the right path, but rituximab isn’t ‘quite,’ the right fit in terms of treatment.
https://www.google.com/amp/s/www.docwirenews.com/condition-center/multiple-sclerosis-knowledge-hub/skewing-of-the-b-cell-receptor-repertoire-in-myalgic-encephalomyelitis-chronic-fatigue-syndrome/amp/
Perhaps it’s because HIV/AIDS got enormous media attention and people were terrified of it. But, that’s when it was new, devastating and little was known about it. It’s because of the massive amounts of funding it had that we know so much more and the disease burden has greatly decreased. So…….it’s place on the disease burden scale and funding should be adjusted accordingly, no?!
“labs are normal you’re just depressed”
and
“fatigued, yeah I’ve been a little tired myself lately”
Heared those before too, together with the frequent “It’s all in your head” and luckily less frequent “I believe you have problems, you sure do, but you need another sort of healthcare (said with a deep disrespect in the voice)”.
The “best” FM variant of “fatigued, yeah I’ve been a little tired myself lately” I heared was “We have pain too, but we chose to not focus on it rather then what you do”.
Seriously? I am one of only four patients of my dentist who asks to not have analgestics (as I feel my poor health doesn’t need any of those if I can avoid it) nor pain killers when she is drilling wholes going to near my gums (seen by where the fillings end on the side between two molars). She says it pains her more to do the procedure then it seems to do me. When looking at the painful face she makes during most of the procedure, I concur.
Note: no single dental nerve is removed and my teeth are quite sensitive too heat and cold, so my dental nerves work well.
I would love to have sort of a pain tollerance contest with those nay saying psychologists to test the veracity of their “We have pain too, but we chose to not focus on it rather then what you do” claim. It would root out any doubt, especially if none is allowed to quit the test if one remains standing.
Some might need years of counceling to overcome this single experience I guess. They’d be baffled how we can survive such. And pain, as I am more ME heavy then FM heavy, isn’t my worst symptom by far.
Note: I know that many have pain far worse then me, so this is not dismissing their suffrance.
End of rant. Sigh.
Excellent Easter Sunday awakening for ME! Christian Murray’s story, the DALYs, and Brendan Rob’s idea for a fact based un-whiney documentary at this time is brilliant. Long COVID is getting much of the attention we with CFS have long missed, and People magazine’s current coverage of Ron Davis and Whitney just hit the stands and the internet. This morning CBS did a special on business leader and philanthropist Adrienne Arsht known for her many wealthy contributions, such as the $30 million which “saved” Miami’s Center for the Performing Arts Center and bought her naming rights. She has a special attachment to University of Miami where Dr. Nancy Klimas researched AIDS and CFS for years. Perhaps some of that energy and those funds could be directed to Nova Southeastern’s Institute for Neuro-Immune Medicine and Brendan Rob’s documentary. The time is NOW!
dejurgen, I hear you
there is no other like you, no ‘doppelgänger’ with your qualities, interests, determination, talents, I am glad to know you thru HealthRising.
And i believe you, and am so glad you are alive. And even if you weren’t willing to run the marathon of disease determination, and discovery, I would be glad still to know you. that so many have discounted you speaks to their lack of understanding, lack of compassion, and lack of discovery; not yours. You build others up at the same time as you confront challenges and puzzles.
In my grandpa’s young days, there was no veterinarians near him and his neighbors. He was inventive and wise, and the neighbors would call on him for help often.
so I want to coin “Theo—Dore”
as a dignified title signifying respect for those with your and my grandpa’s qualities.
(from online definitions, Collins English Dictionary; Baby names, Word origins.)
Theo—brave people
Theodore—gift from God
Dore—coated with gold
Dore—the color ‘golden’
So in short, “Theo—Dore” is likewise a wonderful person worth their weight in gold, with many golden qualities.
The problem there is that pain is another subjective symptom for which there is no one clear bio marker for, especially when it comes to degree of pain (there can be elevated blood pressure and HR, but I suspect that with a high pain tolerance, they may not be as elevated….). That said, that’s incredibly insensitive, condescending and ignorant! Ya, everyone has some pain at some time or another, but not everyone has constant and debilitating pain! I admire your pain tolerance and my heart goes out to everyone with FM!
Hi Ronp and dejurgen, I hear you.
Result of all this is I have to force myself to attend a doctor just to get my bp medication I no longer want to talk about ME/ CFS and FM no point I’m too depleted to make an effort anymore. Take care.
I wish you had a thousand dollars for every time someone said that to you;
Meven more, I wish people would stop saying that to you……..
and at minimum, say instead:
there are things I have not understood, and I am making an concerted effort to become educated about this disease. I am sorry I have not taken you seriously enough, for you do have a serious disease.
Or what responses from them would be better or more appropriate for a truly compassionate response?
(I am hoping that some who at one time did not understand have been pointed to this site, to ‘hear’ how life is for so many.)
Ron P
I wish you had a thousand dollars for every time someone said that to you;
Meven more, I wish people would stop saying that to you……..
and at minimum, say instead:
there are things I have not understood, and I am making an concerted effort to become educated about this disease. I am sorry I have not taken you seriously enough, for you do have a serious disease.
Or what responses from them would be better or more appropriate for a truly compassionate response?
(I am hoping that some who at one time did not understand have been pointed to this site, to ‘hear’ how life is for so many.)
Sunie, I came across this great quote by Goethe: ‘A person hears only what they understand.’ They just don’t understand it.
Tracey Anne (Burgess)
Thank you, that is just what I needed to hear 🙂
I feel that it is every doctors’ responsibility to stay current in their practice. If they don’t know or understand, it is their duty to say so and educate themselves so they can help you. Doctors are too often afraid to say they don’t know, but it’s better to do so than give bad advice. That’s how I always operated in my health field and my patients always appreciated it (and I learned, which in turn helped me help others!). I would even go so far as to say that it is malpractice in a lot of situations.
One thing that I have found helpful when you know have ME/CFS/FM is to bring information (like the 2015 IOM report, primer for practitioners and other similar articles) and actually take a highlighter to it to designate mail symptoms and show that I meet criteria for dx.
The other thing I have done is to complain to the appropriate officials that may be available to help. I saw a sleep specialist re a major flare up of my RLS for months on end. I am well versed in RLS and came with specific questions that were in the context of CFS – could the small fiber neuropathy and/or circulatory issues associated w CFS possibly be contributing factors? All she could do was tell me that since I wasn’t elderly and had never smoked that I couldn’t possibly have those problems, but maybe she could refer me to a vascular surgeon (which is like calling the fire department to blow out a match). I brushed it off until I got an enormous bill. I called the patient advocate and explained my concerns (including the fact that she had charged me for 45 min for a 30min appt, which is fraud….). It resulted in a meeting of the advocate w the doctor and whoever else. The success there is that the doctor was informed and will hopefully learn from it. I am considering doing the same thing with my previous PCP who “thought I knew I had CFS” because somewhere along the line it was added to my problem list (probably related to my major depression) by a provider that clearly did not understand CFS. So, here I was still exercising like a maniac before I figured out I had CFS. If my PCP thought I had CFS all along, she should have told me to STOP! I had no idea I was damaging myself w my continual push/crash cycle. She “believes” in CFS, but obviously was not on top of one of the most important aspects of quelling the disease and giving hope of some recovery with early intervention. Not OK.
I agree with you Wendy. Also I think a bigger problem than – just not understanding, is arriving at the wrong conclusion that the health issues are ‘all in the head’ and so therefore any further search for answers is completely unnecessary. PS, I’d really like you to be on my team!
The organization that I direct, Birth Defect Research for Children, has worked on a very controversial issue for many years….male-mediated birth defects. These are birth defects linked to epigenetic changes in sperm caused by certain environmental exposures that can create health problems that can carry on through generations. Studies have been done, one at a cost of nearly a million dollars, but not accepted for publication. A meta-analysis of 22 studies found paternal exposures to Agent Orange associated with birth defects and yet the results of this analysis were not accepted and nothing has been done to help the affected families.
I believe that the problem with funding for ME/CFS is that some cases (and perhaps many) have been triggered by an environmental exposure. Unless you work in this field, you have no idea the power and pressure there is to “not link” human health problems to toxic environmental exposures.
See this study published last April.
For ME/CFS Patients, Viral Immunities Come at a Devastating, Lifelong Cost
https://health.ucsd.edu/news/releases/Pages/2020-04-27-for-me-cfs-patients-viral-immunities-come-at-lifelong-cost.aspx
For over 20 years, I have served as a chair for the National Institute of Environmental Health Sciences’ Public Interest Partners. This is a group of NGOs (breast cancer, autism, autoimmune diseases, asthma, etc.) where environmental exposures are thought to play a part in the onset of the health problem.
We have conference calls with NIEHS researchers and read the research summaries that come out each month. Connecting any disease to a toxic exposure is a uphill battle.
As I have probably pointed out too many times, reduced immune function opens the door to increases in any of the herpes family viruses: EBV, CMV, chickenpox, HHV-6 (a and b), HHV1 and 2 and so on. A competent immune system also controls bacterial balance.
And Australian farmers are at present
making a great case to keep on broad acre spraying with Gramaxone. For those who don’t know you’ll have to look it up too tired to explain.
I want to commend all of you for your positive attitudes in the face of this.
I’ve been diagnosed with me/cfs for 12 years, but didn’t start accepting it til I had to stop working 2.5 years ago. When I read Cort’s article above, I again feel denial–I don’t want this diagnosis! But here it is. I’m looking to these articles and comments to find a way to be a positive advocate for myself and others. Thank you 🙂
Hi Anne,
This was shared on Twitter earlier it’s a short, beautiful animation about ME/CFS by Inga Topolnicki. Here’s the link:
https://www.youtube.com/watch?v=dUrPFqGONM8
I thought it was stunning.
I think studies like this one by Mirin, Dimmock and Jason are crucial in putting forward the long neglected, desperate needs of individuals suffering daily with ME/CFS. They make their point clearly and effectively. I’m not in the US but as Cort points out and Emily Taylor and Solve M.E. are focusing on – Congress has the power to direct the NIH. Most people in any job, knows who really holds the power – who you need to watch out for. It’s painfully obvious that the NIH are failing US citizens with ME/CFS and it seems that Congress is becoming increasingly aware of this. If the current system within the NIH doesn’t serve its purpose, then isn’t reform long overdue?
In my experience with these kind of issues, pressure needs to be kept up until you’re over the line. It’s hard, gruelling and exhausting but can be worth it in the end. And there seems to me to be so many different and encouraging developments occurring. But still, it’s very difficult for people who suffer pain, isolation, stigma, with little or no support and my heart goes out to everyone.
Betty Mekdeci. What you are saying makes perfect sense to me. The low funding and indifference to get to the bottom of this debilitating disease has got to have people in powerful positions in Big business whose influence extends to control of politicians. The last thing they want to admit to is the interference and weakening of the public’s immune system. Whether it’s a inherited weakened immune system by chemicals people have been exposed to in past or present family members as there does seem to be family’s with more than one person suffering M/E CFS. The other way your immune system can be compromised is the use of corticosteroids ,which if taken by a person when they have an active virus will most likely not clear the virus and the virus gets stronger. The immune system is the great variable when it comes to defeating a new virus such as Covid 19 or keeping the Human Herpes viruses under control that may have reactivated. This is why it takes people various time frames to recover from viral infections and some with weaker immune system and not rested enough or was prescribed corticosteroids for inflammation end up with M/E CFS. The Gist is as Betty Mekdeci says the main problem to begin with is a compromised immune system. Which Big business and there political mates want nothing do with. The obvious reason for no will and no funding!!!
We should remember that there are other organizations that can/do research on ME/CFS. For instance, the Bateman Horne Center has a research program and is very instrumental in providing a large pool of potential research participants, as well as facilitating and coordinating with other researchers. It also occurred to me that the Department of Defense (DOD) does a hefty amount of medical research. Working at the VA for 15 years (until I developed CFS), I saw my share of unexplained ailments suffered by veterans returning from different areas with exposures to who knows what. I did see people w symptoms resembling CFS. It just so happens that one of my state senators is senior chair of the committee on veterans affairs and also one of the top 10 most effective members of Congress. Hmmmmm. Getting ideas…..
Wendy, I’d say you’re a force to be reckoned with!
Cort, thanks for this great article and helpful visuals. Do you happen to have the original high-res charts in PowerPoint or similar? Whitney Dafoe is trying to put together a visually-rich letter campaign to President Biden. He posted about this on Facebook today.
Just got what I had over to him. 🙂
I came down with ME/CFS when I was in my early thirties, and like most of us, was stunned by the medical community’s lack of knowledge. The symptoms were too overwhelming and bizarre to ignore. I was sure they’d get with the program and solve it soon. When the 2009 XMRV fiasco first arose, I thought, “At last!” Nope. Took more than two years to redact that. In 2014, Dr. Naviaux published their study citing that O2 and glucose weren’t being used at the cellular level, and again I thought, at last! We’re now 8 years down the road, with zero treatments. I’m now in my sixties and have spent half of my life (and almost all of my adult life) dealing with the daily symptoms. My ME/CFS still dominates my planning every day. I always figured they’d solve it by the time I got old, and I’d do better than some of my friends in old age. However, I now think they’ll never solve it in time for me, and it is monstrously depressing. None of us get a do-over in life. The better I learn to manage the disease, the less credibility I have with friends and family. So sad.